
Against a backdrop of rising scrutiny of maternity services, increasing intervention rates and a succession of high-profile inquiries, this thought-provoking article by Editorial Director, Neil Stewart explores whether a new rallying call — “No Pregnant Woman Sent Home” — could help rebuild trust between women and maternity services. Examining concerns around triage, admission policies, continuity of care and women’s experiences of not feeling listened to, the article considers whether a simple, patient-centred demand could become a catalyst for wider reform across maternity and midwifery services in England.
How can the safety of women and babies in childbirth be improved and the trust in maternity and midwifery services in the UK restored among pregnant women and those planning their childbirth?
That is the question facing midwifery in England, this article explores a question of whether a new demand for “No women sent home” should be added to prove to all women in childbirth that, as they repeatedly demand, that they will always be listened to and to force the pace of service reform.
The profession has three current urgent policy demands besides the annual pay demand:
- No student midwife left unemployed this summer.
- Meet the extra 3500 RCM midwife recruitment and resources target.
- Close the Midwifery Education pay gap.
But is this enough to move decision makers to reform the place of maternity and midwifery in health services?
The International Confederation of Midwives meet in Portugal this month looking at the global picture. Internationally the profession is strong, demanding a million more midwives across the globe, with WHO and national governments putting midwifery at the centre of their strategies, Women in low income and middle income countries are demanding access to midwives, with midwifery led government policies delivering major improvement in still birth and maternal deaths around the world.
Suddenly the UK looks like an outlier in its debate on maternity services. Defensive, underperforming, resource mismatches, cultural and social challenges. In reality NHS performance is still at the highest levels internationally for safety but improvements have stalled and shocking reports on preventable still births and maternal deaths, the recognition of “birth trauma” and a culture of fear and bullying and racial disparities dominate the headlines and are impacting the views of women toward childbirth in the UK and midwives concerns on what kind of service they are practicing in with a fairly clear increase in defensive medicine.
The public debate on maternity services in England is reaching a crescendo point this June, and the future shape of maternity and midwifery services is in the public firing line.
- Donna Okendon’s next report on Nottingham University Hospitals NHS Trust is reported to be due on 24th June.
- Panorama has been back on the case with a report on 1st June from Michael Buchanan highlighting the consistent issue of women presenting at a unit being sent home with the scandalous notation “FOH” – Fxxxx Off Home – on notes.
- The Today Programme published a report on C-section rates on 5th June from Catherine Burns, health correspondent and Maryam Ahmed, BBC Verify on the rising rate of C-Sections revealing the gobsmacking rise in emergency C-Sections that midwives have been warning of. With emergency caesareans now accounting for around 26% of births in England — more than one in four. When combined with planned caesareans, total C-sections were reported at around 45% of births in 2024–25, overtaking spontaneous vaginal births, far above even the rate in the United States.
- Baroness Amos, commissioned by Wes Streeting to look at 14 units in the news is due to report her findings any time now.
- Kate Brinkworth, Chief Midwifery Officer NHS England published on 23 April with new standards for clinical testing targeting the key issues that account for 52% maternal deaths.
- All this follows previous reports going back a decade including Morcombe Bay, East Kent, Shrewsbury and Telford and now Nottingham with new enquiries running on Leeds and Sussex
Does midwifery face another summer of reports? Adding to the over 80 recommendations already generated but not implemented from previous enquiries and while the service continues going round and around under the same growing pressures: demoralised staff, traumatised women until the next failure produces a scandal and a new enquiry.
Or can this summer of 2026 see policy makers stand back and look at the changes over twenty years in how women give birth, The Lancet Report of 2014, Better Births 2016 , The Renfrew Report 2024 the impact of covid, the extra ordinary rise in C-Sections, the changing choices of women for method of birth, the impact of social media on perceptions of maternity care and midwives, the increasing reporting of birth traumas by women, the entrenched discrimination affecting women of colour and see how the current operating model for maternity units is not fit for purpose.
What can change government policy? It does not look like midwifery can do it alone. There is excellent evidence-based work out there from the original development of Continuity of Care policies, The Lancet Review, rounds of Better Birth strategies, to the Renfrew Report on safety in Oct 2024.
The RCM demand 3500 extra midwives, which the government say they are meeting with 2000 new places so far and an extra £149 million in spending– but managers and educationalists report leavers haemorrhaging from the service and from student courses, feels like they are running up a down escalator.
LMEs, like Nicky Clark formerly of Hull University, highlighting the yawning £15,000 salary gap between NHS scales and Universities posts making education recruitment difficult and now with the added financial panic in universities creating frozen recruitment and even redundancies.
Huge amounts of evidence-based work from the Lancet report of 2014 through the Renfrew report in October 2024 have not been implemented with services running to stand still or even going backwards. Ministers no sooner look up to make a plan than the next media scandal knocks things off course and delayed publication
The government have a task force set up to follow through chaired by the new Secretary of State James Murray. Announced by Wes Streeting its original timetables ran out before last Christmas.
A key issue is that the perceived and reported opinion of women on maternity services is now divided. And in the face of a divided nation of women then policy makers will always reach for the next enquiry to avoid difficult choices.
Gone are the days of “Call the Midwife” levels of trust (not always deserved). The toxic debate around the term “normal Birth” and the allegation that some midwives held back from medical intervention for ideological reasons costing lives seem a distant memory in the face of the prospect of half of all women giving birth by C-sections by the next round of official statistics – the pendulum has swung so far the other way with virtually no public debate or understanding of the scale of change. This is the elephant in the room.
Over the course of the past year a consistent theme has emerged, in fact ever since the first report by Donna Ockendon on Shrewsbury and Telford, that women do not feel listened to by professionals, and midwives have been most in the firing line.
In story after story the midwife, on the frontline is not only the professional working with the woman but the gatekeeper charged by the Maternity Unit to control the flow of “patients” manage capacity, manage beds, make room for the next.
While still births and maternal death come from a range of well-known causes, story after story includes episodes where “the woman was not admitted” the woman was sent home, telephone triage missing what a midwifery visit should have seen. Focussed on in the latest BBC Panorama report alleging “FOH” practices among midwives.
These complaints are even more common in the long tail of birth traumas referenced in the reports which fell short of stillbirth or maternal death.
On a recent Roy Lilley podcast Dr Bill Kirkup, author of the original Morecombe Bay report and enquiry into East Kent reported that the length of stay of a woman in childbirth in a unit was now less that 2 days for the whole process of admission, labour, postnatal support, latching on before discharge.
This has prompted the question among midwives and women as to what happened to “lying in” – the health service maternity capacity to have the space and staffing to bring a women showing unexplained changes, distress, in and monitor her, let the birth take its course and then support her for up to 5 days afterwards while the huge biochemical and physical transformations in the mother and babies bodies start their adjustments.
Lying in can still be seen chipped into the stone doorways of a few older hospitals.
Lying In has a very mixed history, since the post war presumption that a pregnant woman would finish her childbirth in a maternity unit. It was often controlling, hierarchical, the original due date women were given around 39 weeks was as much for NHS convenience to make sure bags were packed, jobs suspended and families ready to support and surround the mother and new baby. (Women give spontaneous vaginal birth across a range of 38 weeks to 42 weeks but that is not a resource pattern that modern bed managed health services find effective).
For the women’s movement and modern women commentators, especially those parts sceptical of medicalisation, having fought from the 1960’s to the 2010s for women’s choice in contraception, abortion and then method of birth, including home birth, waterbirth but in particular the right to request a C-section they are understandably suspicious of calls to bring back things from the past that did not feel like choice for their mothers generation.
The modern NHS mantra as set out by Wes Streeting the former health secretary, “from hospital to community” is for maximum treatment outside hospital, at home with mobile outreach services. But in the case of todays mother and child that too often means, telephone triage, delayed admission then quick discharge into an absent family support system, social isolation with extremely poor post-natal follow up, something the NHS is beginning to recognise with post-natal mental health checks at 8 weeks.
Short stays have merit and are ideal for many pregnant women but not all, and among this later group are many of the missed signs, not supported not monitored adequately that turn into the tragedies.
The Renfrew Report lays out a desired pattern of properly resourced maternity services and the time needed to transition to them ( home births, Midwifery units, alongside units and high risk or emergency Maternity Unit) giving women the choices they say they want, and matched to their risk assessment, but with facility for escalation if that risk assessment changes.
Recent discussions have highlighted how the risk assessment of high risk (age, weight Diabetes, co-morbidities etc) or low risk are often set for a woman at the start of their pregnancy meetings and then baked in and not reviewed, sometimes till it is too late.
So, what needs to be lined up in a row for politics and policy makers to invest in that modern view of maternity services?
The current public narrative dominated with scandals and mistrust of professionals, with its blame culture, fear of birth trauma, with midwives caught in the middle does not point to an optimistic outcome, but just more enquiries and reports.
“No Pregnant Woman Sent Home”
Campaigners have been trying to work out how midwifery can align itself clearly with what women want. To give the policy makers the push and the confidence to change things.
The suggestion is to add to the list of demands, on Midwifery Graduate Student Employment, Midwifery Numbers and Education Pay Gaps the demand that “No pregnant woman should be sent home” shortened to “No Pregnant Woman Sent Home”.
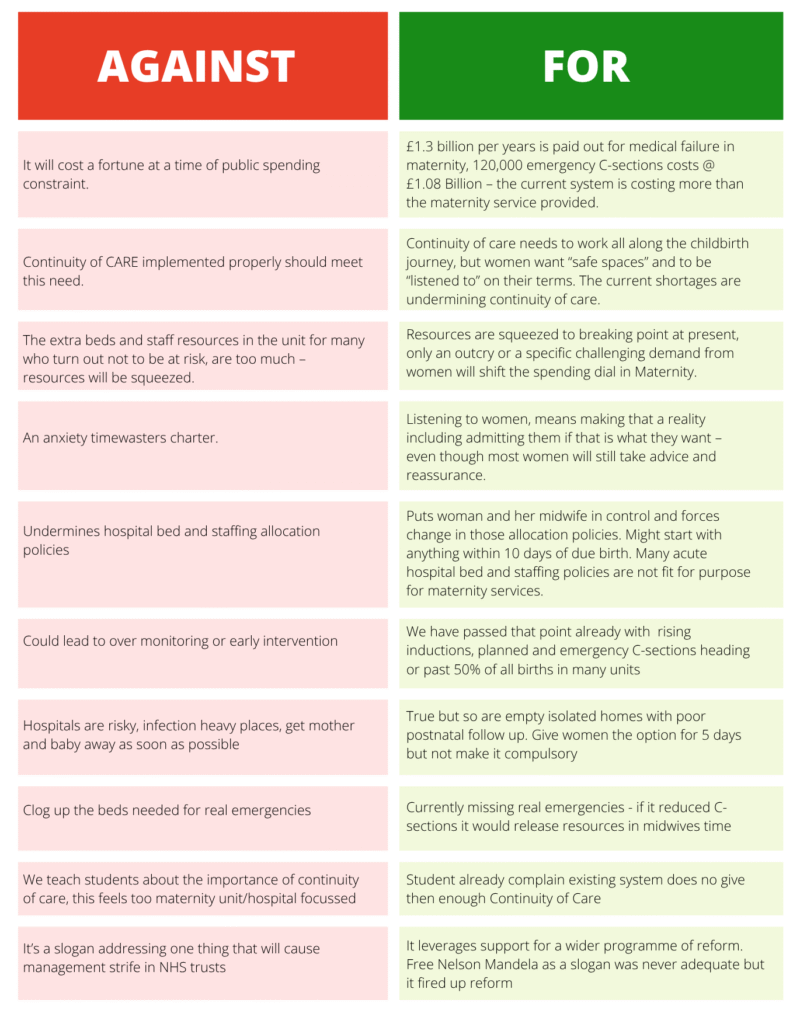
Vote below on whether you think such a slogan should be adopted. Here are some of the arguments for and against as reported to this editor.
No Pregnant Woman Sent home
Neil Stewart, Editorial Director, Maternity & Midwifery Forum
June 2026